







This factsheet will initially explain the normal process of breathing. It will then describe the normal responses of coughing and choking as mechanisms to protect the airways, before discussing how these processes can be affected when you have MSA. Breathing can be affected by several factors. Many illnesses and medical conditions, including Multiple System Atrophy (MSA), may cause changes to breathing. In MSA the lungs themselves and the tissue that extracts oxygen from the air, is healthy. However, the mechanism of breathing and moving the air in and out of the lungs may be affected.
How we Breathe
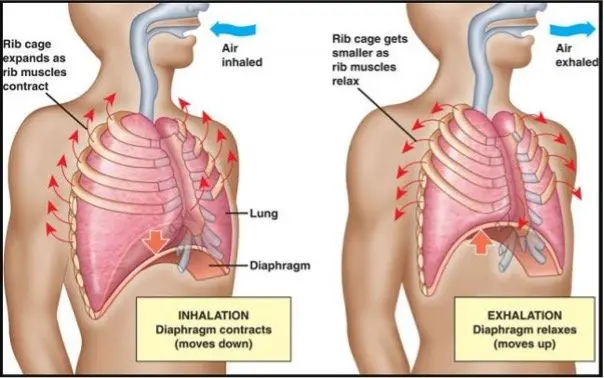
The process of breathing involves how air is moved in and out of your lungs. The diagram below shows the flow of air being taken into the lungs. The lungs take out the oxygen from the air and pass it into the blood circulation to get to all the body cells. The lungs sit within, and are attached to, the ribcage and the diaphragm (the muscle that stretches across the top of the abdomen below the ribs). Breathing in gets oxygen to all the body cells. Breathing out gets rid of the carbon dioxide the body cells produce – this cycle of oxygen in, and carbon dioxide out is the process of respiration.
Most adults when resting or just moving around with little extra effort, will take 12-20 breaths a minute. Activities using our limb muscles more energetically will require more oxygen so our heart and breathing rate will increase. The depth of breathing will improve when we are more active.
The whole length of this breathing tract (passageway) from our nose and mouth down into the lungs, is lined with delicate membranes. These are protected by mucus and very fine hairs to shield the tract from damage and particles that may irritate the airway.
To take a breath the muscles along the whole tract, and in particular the muscles between your ribs and the diaphragm, work together. These muscles tighten pulling the diaphragm down and the ribs down and out, which enlarges the lungs. This pulls air into your lungs – inhalation. Relaxation of these muscles pushes air out of the lungs allowing breathing out – exhaling.
Breathing is controlled by the autonomic nervous system. The respiratory (breathing centre) is in the brain stem where most autonomic function control is located. As blood passes through the brain stem it monitors the oxygen and carbon dioxide levels and adjusts our breathing rate accordingly.
Coughing
Coughing is a normal response to clear secretions from the airway. When we cough we take a big breath in, the top of our airway closes, tummy muscles tighten which puts pressure on the diaphragm. The top of the airway then opens to allow a forceful push of air out and in the process this should clear anything such as secretions or mucus that has built up in the airway. Any food or drink that may have slipped down the wrong way (this is known as aspiration) should also be cleared. See below for more on this.
Choking
Choking is very distressing for the person who is choking and those around them. Choking can happen to anyone when particles of food, drink or other ‘foreign-body’ accidently enters the top of the airway. A reflex coughing spasm is triggered which is usually enough to clear the problem.
In the situation where someone is choking standard first aid measures should be taken.
What should I do if someone is choking? – NHS (www.nhs.uk)
When someone with MSA seems to be having regular episodes of coughing whilst eating or drinking it is essential that they have an urgent review by their speech and language therapist (SaLT) to assess their swallow. It is very rare for someone with MSA to die from choking, particularly if they follow the advice their SaLT provides. This advice may include modifying the size, texture and consistency of food and drink if chewing or swallowing is difficult.
How may MSA affect your breathing?
One of the more common breathing problems for people with MSA is caused by chest infections. These are often due to a combination of aspiration, poor lung expansion and build-up of secretions that can be difficult to clear.
Aspiration occurs due to altered co-ordination of swallow that allows food particles, drips of fluids or saliva to slip into the top of the airway. Normally saliva is produced near the front of the mouth and the tongue and cheeks move it round the mouth and to the back of the mouth which then triggers a spontaneous swallow. This spontaneous swallow occurs less frequently for people with MSA and may be poorly co-ordinated. When this occurs saliva (or any food or drink particles) may slip into the airway instead of going down the food pipe into the stomach. You can read more about saliva in our ‘Saliva and MSA’ factsheet.
Poor lung expansion often occurs in people with MSA because movement is slowed and restricted. Reduced mobility means breathing becomes more shallow and the lungs do not fully expand.
Your physiotherapist can advise on exercises you can do to increase lung expansion called lung volume recruitment exercises. These exercises can also improve the strength of your cough to clear secretions. In some areas you may be able to access a specialist Respiratory Physiotherapist who has particular expertise to assist people with breathing difficulties.
Postural changes can impair the chest movement. Sitting up as straight as possible helps the diaphragm and ribs to move freely, to expand the lungs better and improve air intake. Your physiotherapist and occupational therapist will be able to advise you on posture and look at adapting support in your chair to help maintain a good posture. Sitting in a well supported position is important when eating too as this will reduce the risk of food and drink slipping down the wrong way and causing aspiration.
Reflux and/or heartburn can cause the sensitive lining of the food pipe to be irritated by the regurgitated acid from the stomach into the food pipe. The lining then gets inflamed and produces more secretions to try to protect itself – these extra secretions can build up and slip down the airway too. Eating smaller regular meals, staying sitting upright for at least 30 minutes after a meal and avoiding eating too close to bedtime can all reduce the risk of reflux. It can be helpful to take an anti-reflux medication too.
Secretion build-up can be a really frustrating and irritating symptom. Constantly trying to clear secretions can be tiring. Anything that irritates the sensitive lining of the airway can cause extra secretions to be produced e.g. aspiration of saliva, food, drink, reflux, very cold or dry air, irritant particles in the air.
If the secretions are too sticky it can be very difficult to cough them up and either clear them away in a tissue or swallow them. To help keep secretions loose and easy to clear it is important to keep well hydrated.
This is particularly important when you have a chest infection as this will cause more and thicker than usual secretions.
Putting into practice the lung volume recruitment exercises and cough techniques can help improve the clearance of the secretion build up.
In some cases if you have a persistent problem with clearing secretions and they are thick and sticky you may be prescribed a medication that breaks down the stickiness called Carbocysteine / Mucodyne. You may be given a nebuliser (a pump that pushes air through liquid) that gives vapourised air through a face mask.
Occasionally if the doctor thinks your airways are so irritated they are inflamed and narrowed you may be prescribed an inhaler or nebuliser with medication that opens up the narrowed airways.
Suction machines can be provided in some specific situations when you can get the secretions to the back of the throat but can’t manage to swallow and clear them away or bring them forward into the mouth to clear them. A carer or partner would need some basic training to use the suction machine. It should only be used to clear secretions caught at the back of the throat if they are causing distress and can’t be otherwise cleared.
Carrying out suction beyond the back of the throat into the airway should only be done by qualified nurses or physiotherapists. This would usually be in a hospital setting when someone is being treated for an acute chest infection. Overuse of suction can irritate the airway causing more secretions to be produced or dry it out too much and so becomes counter effective.
Cough assist machine – In some circumstances when a person has a very weak cough and can’t manage to take deep enough breaths in to stimulate a cough to clear secretion, they may be offered a machine called a ‘cough assist’.
This machine is usually provided by the respiratory team and you and your carer or partner would need to be trained how to use it. The cough assist machine gives short episodes of pressurised air via a face mask to build up enough air in the lungs to induce a cough. It then quickly pulls the air back out which helps clear any accumulated or thick secretions. You will need to learn how to control your breathing to ‘work’ with the cough assist and get used to the feeling of air pressure building up. A cough assist can be a very useful device and can be used on a regular daily basis almost as a form of chest physiotherapy to assist better lung expansion generally.

The cough assist is not widely available and you would need to be formally assessed as needing it. There are a number of different machines available so they may look different but they all do the same job.
Obstructive Sleep Apnoea (OSA)
Obstructive sleep apnoea (OSA) is quite common over the age of 40 years. Any of the following factors can increase the risk of someone developing OSA – being overweight, smoking, drinking alcohol in the evening or taking sedatives. There is an increased risk of OSA in MSA due to damage caused by the MSA process to the autonomic nervous system. This damage can cause changes to the initiation of breathing and to the co-ordination of the muscles along the airway.
Obstructive sleep apnoea occurs when we are asleep. Initial signs may be an increase of noisy snoring. It is often reported by partners, who may also observe a change in breathing pattern when the person with MSA is asleep, noticing an irregular pattern and short periods of snorting, gasping or not taking a breath. This cycle may be repeated frequently throughout the night.
The change in breathing noises occurs due to the muscles and tissue of the throat and top of the airway relaxing and collapsing on themselves so partially or totally blocking the passage of air momentarily. When this happens the brain breathing centre detects inadequate breathing and rouses you from restful deep sleep to a lighter sleep or wakefulness which reopens the airway and allows normal breathing. When this cycle is occurring frequently every night, even though you are probably unaware of it happening, it can leave you feeling very tired the next day.
If you are experiencing OSA then discuss this with your GP or Consultant who may refer you for a sleep study tests. It can be helpful if you have a family member who can record your breathing pattern and noises when you are asleep. This can be very helpful to the doctor to determine what the problem is and the range of further tests required.
For the sleep study test you may be given an oxygen monitor probe to attach to your finger overnight with a recording box or a breathing and heart rate monitor to wear overnight. In some cases you may be asked to stay overnight at a hospital sleep study centre where a more complex range of skin sensors are used to monitor your muscle movement, breathing, heart rate, oxygen levels, snoring and brain wave patterns – this is called polysomnography.
The results of the monitoring will determine whether treatment is required. For some people changing the position they are sleeping in can be enough to keep the airway open, lying on your side rather than your back for example.
Continuous Positive Airway Pressure (CPAP) is the main treatment offered. This is a small box which contains a pump that compresses air.

Attached to the pump is a tube which connects to a face mask that you wear overnight. There are a number of different masks you can try to find the one that works best for you.
The pump pushes compressed air into the airway. The pressure is set by the sleep centre that provides the CPAP machine, at a level that is enough to stop the throat and upper airway tissues collapsing down and blocking your airway. Many people find using CPAP takes some getting used to, so it is advised to gradually build up the time you use it for. Adjustments can be made to the settings and masks if necessary. Most people do get used to using the CPAP and find they sleep better. They often say they feel more rested the next day and more energised to do things.
Central Sleep Apnoea
Earlier in this factsheet we mentioned how the autonomic nervous system is involved in breathing by co-ordinating some of the muscles involved in breathing and importantly by monitoring the amounts of oxygen and carbon dioxide in the blood. The balance between these gases stimulates breathing. The monitoring centre is in the brain stem and for a small number of people with MSA this respiratory monitoring centre can become impaired by the MSA process, causing breathing to fail and resulting in death that may have been unexpected at that time. There is no way of anticipating who this may happen to or when, and there are no medical interventions to protect against this.
If the respiratory monitoring centre fails it often occurs whilst the person is asleep in their own bed, so although death is sudden and not foreseen it is usually peaceful.
Stridor
Stridor is a very specific sort of breathing noise that some people with MSA can develop. It is a tight, high pitched rasping or wheezing sound most commonly on breathing in but can be on breathing out too. It is suggestive of a significant obstruction in the airway, in MSA this is usually due to vocal cord spasm. The cords which are either side of the top of the airway should fully open and close in unison. Due to the autonomic damage in MSA in some people this causes abnormal movement or lack of movement in the vocal cords, restricting the flow of air past them.
Usually a stridor may initially be noticed during sleep – and again recording of the noise is helpful to determine this. Over time it may well become apparent during waking hours too.
As soon as you are aware of unusual noisy breathing you should contact your GP and if stridor is suspected they will arrange an urgent assessment by the Ear, Nose and Throat Specialists or the respiratory team. Treatment will depend on the specialist assessment of what is happening.
Treatment will most likely require CPAP as described above. In some cases, if there is difficulty with breathing out as well as breathing in a very similar looking pump to the CPAP called BiPAP may be used. This helps push air in past the restricted vocal cord movement and helps draw air back out. Sometimes the same box has both settings on it so can deliver CPAP or BiPAP.
Tracheostomy
In a few cases the specialists may feel the vocal cord movement is so impaired that you would be better to have a tracheostomy. This would be discussed with you but it will be your choice.
A tracheostomy is a small opening made in the front of your neck where the soft indent is just below your Adam’s apple. The opening goes through the skin and cartilage into your airway (trachea) below the vocal cords. This allows you to get air in without the vocal cords restricting the flow. The opening in the neck is usually kept open by a small silver or plastic tube. The skin around the opening and the tube itself requires particular care.
You, and any supporting family or carers will need to be shown how to manage this by the hospital team that carry out the tracheostomy before you can go home.
In rare instances someone with MSA may develop a sudden vocal card spasm or paralysis. This would cause sudden stridor and obvious difficulty breathing. In this situation call 999. In these circumstances an emergency tracheostomy may be inserted unless you have previously had a discussion about having a tracheostomy and made it clear that you would not wish this to be done even in an emergency. This would be an advance decision to refuse treatment and should be documented as part of your advance care plan and be readily available to the medical team treating you. You can find out more on this in our Planning for the Future resource – https://www.msatrust.org.uk/support-for-you/for-people-affected-by-msa/planning-for-the-future/.
Anaesthetic and MSA
People with MSA are often concerned about whether it is safe for them to have an anaesthetic for a surgical procedure. Many people with MSA do undergo surgery with anaesthetic successfully and uneventfully every year. As with so many aspects of life with MSA, most things are possible with good planning, and this is the case with having an anaesthetic.
Why do you need an anaesthetic?
The following three scenarios are the most likely to justify considering having an anaesthetic:
- Is the surgery being done due to a life-threatening emergency? You can’t plan for this and the medical team will do their best with the information to hand.
- Is the surgery needed to treat a life threatening condition but is planned so you or family are able to discuss implications and concerns and advise the surgeon and anaesthetist that you have MSA?
- Is the surgery to address a troublesome symptom that is undermining your quality of life?
The next consideration is whether you need a general anaesthetic or whether the procedure is possible using a spinal or epidural, local nerve block or local anaesthetic. These discussions need to be had with the surgeon and the anaesthetist to identify the safest and best way forward.
If a general anaesthetic is required, then you should have a full pre-operative respiratory assessment and support from physiotherapy to practice breathing techniques. To assist recovery after the anaesthetic, support from the physiotherapist to encourage good deep breathing and clearance of any secretions, is needed.
Key points to remember
- Ask your physiotherapist to show you how to do lung volume recruitment and cough exercises.
- If you have changes to overnight breathing or increased noisy breathing in the day ask your doctor about having a sleep study done.
- If you use a CPAP machine but find the mask uncomfortable ask the centre you got it from if you can try a different type of fitting for this.
- Contact the Speech Therapist if you are needing to clear your throat repeatedly or coughing when you are eating or drinking as you may need a swallow review.
