







There can be several issues affecting sleep in MSA. In this factsheet we look at Rapid Eye Movement (REM) sleep disorder, Sleep Apnoea, Stridor, Nocturia, Restless Leg Syndrome (RLS), Insomnia, Confusion, Daytime Sleepiness and Sleep Hygiene.
Normal Sleep Pattern
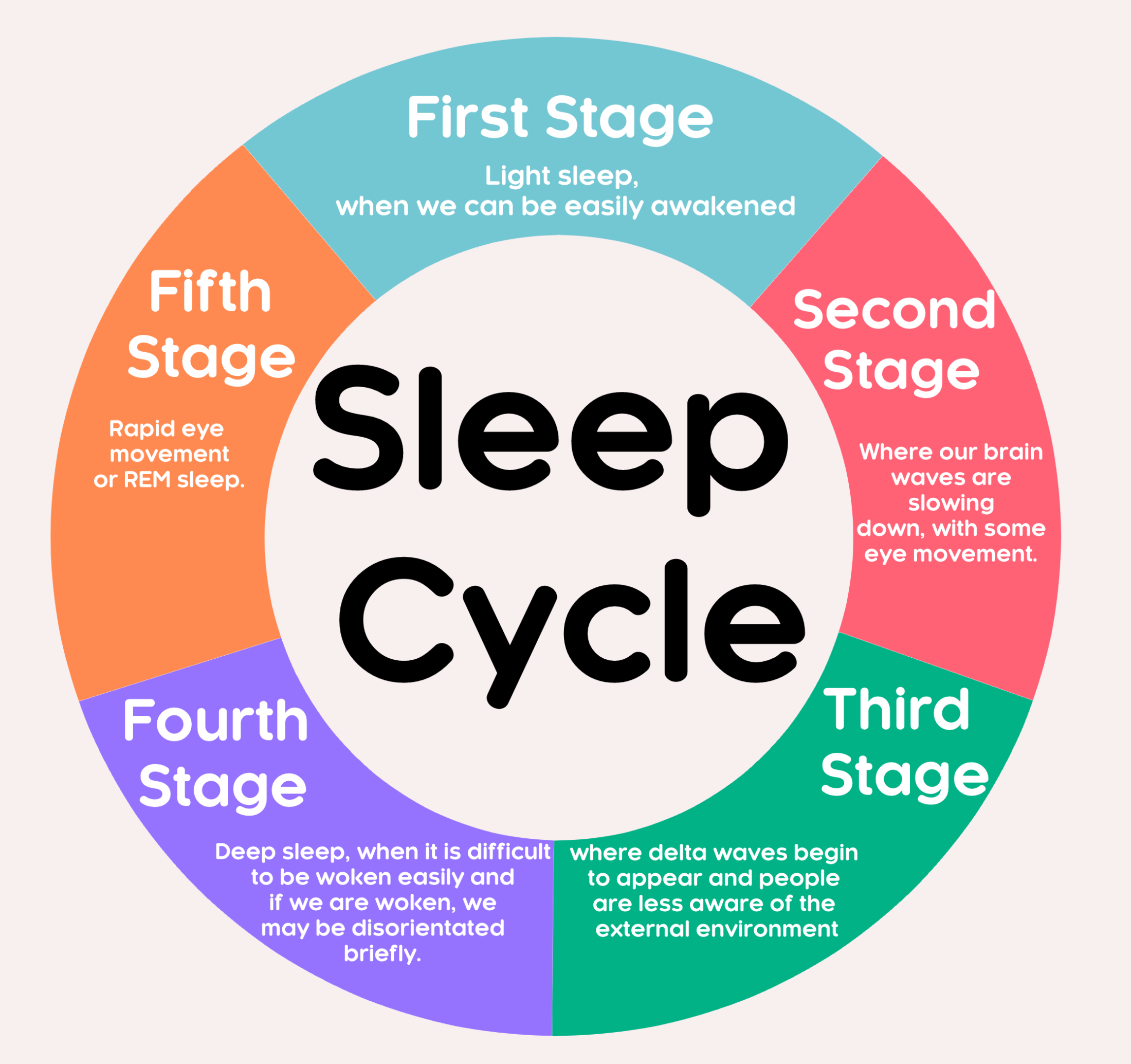
In health, our sleep consists of five stages. These are outlined in the image below.
REM Sleep Behaviour Disorder (RBD)
REM sleep behaviour disorder (RBD) can manifest as small muscle twitches and quiet sleep talking to loud shouting, punching, kicking, grabbing a bed partner and jumping out of bed. Dreams associated with RBD are often intense and frightening. People may dream about being chased or attacked, and they can unknowingly enact the dream in real life.
RBD symptoms can include:
- Minor movements of the limbs.
- More pronounced body movements such as punching, flailing, kicking, sitting up in bed, or jumping out of bed.
- Vocalisations including talking or shouting.
People with RBD are not aware of these behaviours during episodes, and in fact, many people only find out that they have RBD when they are told about their symptoms by a bed partner.
When a person is having an episode, they can usually be woken relatively easily. When they wake up, they are usually alert, coherent and can recall the content of the dream. Episodes can occur once or multiple times during the night. People may experience them a few times per year or every night. RBD can develop suddenly or gradually, but symptoms typically worsen over time.
The condition usually requires treatment because it increases the risk of injury to the person with MSA and their bed partner and can cause fatigue, making MSA symptoms worse.
Causes of RBD
It is thought that dysfunction and degeneration of specific regions of the brain cause RBD, including the brainstem. This area is also responsible for postural instability and freezing of gait, symptoms which are seen in MSA.
RBD can come before the development of neurodegenerative diseases like MSA.
Complications of RBD
Due to the potentially violent nature of their movements, individuals with RBD can put themselves and their bed partner at risk of physical injury. Even when the potential for physical injury has been reduced, the disruption of sleep to the individual or their sleep partner can still lead to potential relationship issues.
If you or your partner think you may have RBD, consult your GP or discuss this with your Specialist. They may then refer you to a sleep centre for some tests. Typically, the sleep centre will carry out a physical and neurological examination. They will rule out potential causes such as alcohol, medications or narcolepsy. You may be referred for an overnight sleep study. During the study (non-invasive) sensors monitor your breathing, eye movements, arm and leg movements, brain and heart activity and blood oxygen levels. It is common to record any dream enactment behaviour.
RBD Treatments
The treatment for RBD is tailored to an individual and can involve a combination of lifestyle changes, medication and injury prevention techniques.
Avoiding Triggers
Because the use of certain alcohol or prescription drugs can contribute to RBD, making lifestyle changes to reduce or eliminate their use may be part of a person’s treatment. These changes can be part of a larger set of steps to improve sleep hygiene, such as setting a consistent sleep schedule.
Medications
Melatonin may be the first medication suggested for RBD. It usually has fewer side effects than other medication options but has similar effects. It can be a safer option for older people, people with dementia, people at risk of falls, or those with sleep apnoea. The dosage of melatonin one should take for RBD is different than when taking it to fall asleep, and a sleep physician will advise on dosage.
Clonazepam, a muscle relaxant drug, is effective in reducing symptoms for 50-80% of people with RBD. However, it can cause some side effects including sleepiness, forgetfulness and impaired balance in the morning. In some cases it can also worsen sleep apnoea, so it should only be used under the guidance of your specialist. They can best advise you on a treatment plan based on your medical history and symptoms.
A safe environment
Establishing a safe sleeping environment should be considered with RBD. Sleep-related injuries including bruising, cuts, fractures and blunt trauma can occur. In addition, the bed partner is also at risk of injury when they are sleeping next to someone who unknowingly acts out violent dreams.
Recommendations for injury prevention if the thrashing around is severe, may include:
- Removing sharp objects from the bedroom
- Placing padding on the floor around the bed
- Installing padded bed rails on the side of the bed
- Putting the mattress on the floor
- Moving furniture and clutter away from the bed
- Padding the corners of furniture in the bedroom
- Protecting bedroom windows.
If the individual shares their bed with a sleep partner, they may prefer to sleep in separate beds or separate rooms until symptoms are well treated.
Sleep apnoea
Sleep apnoea is the involuntary stopping of breathing while someone is asleep.
There are three types of sleep apnoea – Obstructive sleep apnoea (OSA), Central Sleep Apnoea and a mixture of the two. OSA is the most common. Someone who is overweight is more likely to have obstructive sleep apnoea.
In OSA disruptive breathing occurs because of a narrow or blocked upper airway, associated with the soft tissue of the mouth and throat. During sleep, when our throat and tongue muscles are more relaxed, this soft tissue can cause the airway to become blocked, which leads to broken sleep and a disturbed oxygen balance in the body.
During the day we have sufficient muscle tone to keep the airway open. When we experience an episode of apnoea during sleep our brain will automatically wake us up, usually with a very loud snore or snort, in order to start breathing again.
In central sleep apnoea, the problem isn’t a blocked airway. Instead, pauses in breathing occur because the brain and the muscles that control breathing aren’t functioning properly. This can be either a lack of respiratory muscles activating or the brain failing to ask the respiratory muscles to activate.
To breathe in, our brain sends a signal to the diaphragm and the muscles of our rib cage to contract. The contraction of the diaphragm and rib cage muscles produces an inhalation. In central sleep apnoea there is typically a lack of communication from the brain to these muscles.
The prevalence of sleep apnoea increases with age. Symptoms include snoring, gasping, choking and shortness of breath. People with movement disorders such as MSA are 20% (or 2 in every 10 people) more likely to develop sleep apnoea than the general public.
These periods of ‘stopping breathing’ only become clinically significant if the stopping lasts for more than ten seconds each time and occur more than five times every hour.
How do I Know I Have Sleep Apnoea?
People with sleep apnoea may complain of excessive daytime sleepiness often with irritability or restlessness. But it is normally the bed partner, family or friends who notice the symptoms first. People may experience some of the following:
- Extremely loud heavy snoring, often interrupted by pauses and gasps
- Excessive daytime sleepiness, e.g. falling asleep at work, whilst driving, during conversation or when watching TV
- Irritability, short temper
- Morning headaches
- Forgetfulness
- Changes in mood or behaviour
- Anxiety or depression
- Decreased interest in sex.
Diagnosing Sleep Apnoea
This will usually involve a night in hospital where equipment will be used to monitor the quality of your sleep. The results will enable a specialist to decide on your best course of treatment. The ultimate investigation is a sleep study (also known as polysomnography), which will include:
- Electro-encephalography (EEG) – brain wave monitoring
- Electromyography (EMG) – muscle tone monitoring
- Recording thoracic-abdominal movements – chest and abdomen movements
- Recording oro-nasal airflow – mouth and nose airflow
- Pulse oximetry – heart rate and blood oxygen level monitoring
- Electrocardiography (ECG) – heart monitoring
- Sound and video recording.
Treating sleep apnoea
The primary treatment for sleep apnoea is the nightly use of continuous positive airway pressure (CPAP). A CPAP machine blows air at pressure into your upper airway through a mask worn over your mouth or nose at night. The mask is attached to tubing connected to the CPAP machine. CPAP treatment helps to keep your upper airway open while you are sleeping. This prevents obstruction and improves oxygenation during sleep. Polysomnography may be repeated to confirm the effectiveness of CPAP. Many adults have difficulty tolerating a CPAP device at first and may require repeat adjustment and instruction for best fit and correct use.

Stridor
Stridor is an abnormal high-pitched sound on inspiratory breathing, produced by turbulent airflow through a partially obstructed airway It may be harsh, musical or breathy. It is different from stertor, which is a lower-pitched, snoring-type sound.
Stridor is usually caused by a blockage or narrowing in the upper airway. In MSA, stridor may occur as a result of the vocal cords not functioning normally, rather than an obstruction. If you experience stridor your GP or Specialist will refer you to an Ear Nose & Throat (ENT) surgeon, who will look at the vocal cords under sedation to see if there are problems with the cords being too floppy or too rigid. If the cords are rigid, Botox injections may be helpful. If the cords are floppy or paralysed, they may advise a tracheostomy.
Tracheostomy is a surgical procedure which consists of making an incision (cut) on the anterior aspect (front) of the neck and opening a direct airway through an incision in the trachea (windpipe). A tube is inserted to keep the airway clear. Stridor may be a medical emergency. Please see our ‘Breathing and MSA’ factsheet for more information on Stridor.
Restless Legs Syndrome (RLS)
Restless legs syndrome (RLS), also called Willis-Ekbom Disease, causes unpleasant or uncomfortable sensations in the legs and an irresistible urge to move them. The sensations may be described as aching, throbbing, pulling, itching, crawling or creeping. RLS symptoms may vary from day to day, in severity and frequency. Symptoms commonly occur in the late afternoon or evening hours and are often most severe at night when a person is resting, such as sitting or lying in bed. They also may occur when someone is inactive and sitting for extended periods.
Moving the legs or walking typically relieves the discomfort but the sensations often recur once the movement stops.
In most cases the cause of RLS is unknown. 10% (or 1 in 10 people) of the general public experience RLS. However, there is a genetic component that can be found in families. Evidence indicates that low levels of iron in the brain also may be responsible for RLS.
Evidence also suggests that RLS is related to a dysfunction in one of the sections of the brain that control movement (called the basal ganglia) that use the brain chemical dopamine. Dopamine is needed to produce smooth, purposeful muscle activity and movement. Disruption of these pathways frequently results in involuntary movements and people living with MSA have an increased risk of RLS. Treatment is often with dopamine agonists, medication such as Ropinirole or Pramipexole.
During an episode of restless legs syndrome, the following measures may help relieve your symptoms:
- Massaging your legs
- Taking a hot bath in the evening
- Applying a hot or cold compress to your leg muscles
- Doing activities that distract your mind, such as reading or watching television
- Relaxation exercise such as yoga or tai chi
- Taking magnesium supplements/ using magnesium spray to leg muscles
- Walking and stretching.
Lifestyle changes can also help including cutting down on alcohol, caffeine, treating anaemia etc.
Nocturia
Nocturia is waking up at night with the urge to urinate, characterised by an increased sense of urgency, hesitancy and increased frequency. We shouldn’t need to get up overnight to pass urine, it is normal to be able to control the bladder for eight hours overnight, even as we age. As the urinary system and mobility can be affected in MSA some people find that they can’t control their bladder and can’t get to the toilet in time.
Some medications can cause nocturia, for example some anti-depressants or medications for high blood pressure. Other treatable causes such as infections, prostate difficulties (in men), and other renal or circulatory dysfunction should be ruled out.
Another cause of nocturia is low blood pressure (postural hypotension) commonly seen in MSA. When blood pressure is low, it doesn’t perfuse the kidneys with blood, so urine isn’t produced. When we lie down at night the blood pressure rises naturally, blood flows to the kidneys and more urine is produced.
See our factsheet on postural hypotension for further information.
If you are experiencing nocturia, ask your GP, specialist or Parkinson’s Nurse Specialist (PDNS) to refer you to a Urologist for an assessment. They can suggest ways to treat and manage the issue.
You may also be referred to a continence advisor – a specialist nurse who assesses and manages bladder and bowel issues.
Treatment of Nocturia
A urologist will look at your symptoms and consider other possible causes such as kidney problems, diabetes, high blood pressure, congestive heart failure, obstructive sleep apnoea or prostate issues in men. There are several medications that may help.
You may be prescribed an anticholinergic medicine to treat bladder muscle problems. These are used to correct an overactive bladder that may go into spasm. Examples include solifenacin, tolterodine or oxybutynin. Another medication you may be prescribed is mirabegron which causes the bladder muscle to relax, helping to prevent urgency, frequency or uncontrolled urination.
In some cases, the hormone desmopressin (DDAVP) taken as a nasal spray at bedtime may be helpful to help the kidneys produce less urine overnight.
All of these medications can cause side effects so ask about these when they are prescribed, so you know what to look out for. If you are prescribed DDAVP you will need to have regular blood tests at your GP surgery as it can affect the Sodium and Potassium levels in your bloodstream.
MSA can cause several urinary issues, not just nocturia, please see our ‘Bladder and MSA’ factsheet for more information.
A continence nurse specialist can advise on bladder and bowel issues. They can carry out a portable ultrasound of the bladder to see if it is emptying properly. They can also suggest equipment or aids that may help to manage continence.
If you are having problems sleeping because of an increased urge to pass urine at night, you may want to try the following:
- It is important not to cut down too much on the amount of fluid you drink. This may leave you dehydrated and may make the bladder more irritable. But try and reduce the amount you drink in the evening and make sure you have been to the toilet before you get into bed
- Avoid drinking alcohol or caffeine-containing drinks, such as coffee and tea, in the evening and try to limit these during the day generally
- You might want to try absorbent sheets and bed pads, just in case. Appliances such as urinals or sheaths (used by males) may also help you if you are having problems getting to the toilet. The continence advisor or community nurse can advise and supply these
- If you are prescribed a diuretic take it at least six hours before you go to bed
- Elevate your legs whilst you are sitting, especially in the evenings and wear elastic compression stockings as these help to prevent fluid build-up
- Empty your bladder before setting down to sleep at night
- Try an afternoon nap. When you sleep poorly, a nap can be help you feel better during the day. Naps can also allow liquids to be absorbed into the bloodstream. However, be careful not to nap too long. Aim for 30-45 minutes, as any more can disrupt your night-time sleep pattern.
Insomnia
Insomnia is a sleep disorder that causes problems getting to sleep or staying asleep at night, so you are likely to feel tired during the day.
If you are having trouble sleeping, a cycle can develop. If you can’t get to sleep, then you can become irritated, fed up or anxious about how you will cope the next day.
These feelings tend to make you more alert, which keeps you awake, and so on. For many people, this is the start of insomnia.
People with MSA can be more prone to insomnia because of Parkinson’s symptoms, such as tremor, stiffness, pain and restless leg syndrome, that can all disturb sleep.
Some medications can act as stimulants and keep you awake. Speak to your GP, Specialist or PDNS for advice about Parkinson’s symptoms or medication if you think these are stopping you from sleeping.
Night-time Hallucinations, Psychosis and Confusion
These are not usually seen in MSA and if they do occur, it is most likely to be caused by something else.
These are not usually seen in MSA and if they do occur, it is most likely to be caused by something else. Night-time hallucinations, confusion and psychosis may result from any combination of cognitive impairment, Parkinson’s medications, age, Parkinson’s related vision changes and/or lack of sleep. Psychosis may also be caused by an acute infection, trauma, surgery, or prolonged hospitalisation. Symptoms may range from a sensation that someone or something is standing at the side of or behind the person, to very detailed and often frightening visions. If any of these occur speak to your GP, PDNS, or the MSA Health Care Specialists for support. There are treatments that can help and these symptoms are usually short lived.
Excessive daytime sleepiness
This is also known as daytime hypersomnolence. Parkinson’s medications can cause excessive daytime sleepiness or sudden onset of sleep. In some cases, this can be severe. It is more likely in people with later stage MSA who are on multiple medications. It can also occur when increasing medication, particularly dopamine agonists. Excessive feelings of sleepiness during the day can also happen if you are not getting enough sleep at night. The effect can cause people to fall asleep or doze off during normal waking hours. This can be dangerous if you are doing certain things, such as driving or operating machinery. Medication may help, so speak to your GP, specialist or PDNS.
Difficulties turning over in bed
Turning over in bed can be difficult for people living with MSA due to rigidity and muscle stiffness. Changes to your medication may help with this, so speak to your specialist or PDNS. Using satin pyjamas or satin sheets may also help. The shiny material can help you to turn over but don’t use satin sheets and satin pyjamas at the same time. Together, they can increase the risk of sliding out of bed too quickly. You might like to try a slide sheet or a grab rail that fits under the bed. An occupational therapist (OT) can provide you with this type of equipment, advise you on beds and mattresses and how to use these.
See our factsheet on Equipment on our website.
Steps to Sleeping Better – Sleep Hygiene
There are some steps you can take to try to improve your sleep. Sleep hygiene may be helpful when dealing with insomnia and daytime sleepiness. Sleep hygiene refers to the behaviours and habits that affect our bodies day-night cycles.
- Try to set and follow regular bed/sleep and wake times with a goal of spending at least seven but not much more than eight hours in bed each night. Bedtimes should be chosen based on a target waking time (e.g. don’t go to bed at 8pm if you don’t want to be up at 4am!).
- The bed should be used only as a place of sleeping or sex. Reading, using a computer and watching television should be done elsewhere.
- Daytime napping should be limited to one nap of approximately 30 minutes, as longer naps don’t provide any greater benefit to daytime fatigue and can disrupt sleep for the coming night.
- Try to expose yourself to as much daylight and physical and mental stimulation during the day as possible. Light is an important synchronizer of the sleep-wake cycle and people with long term conditions tend to have reduced exposure to bright light.
- As physical and mental activity stimulates the alerting and wakefulness centres in the brain and increases blood and oxygen flow to the brain, avoid physical and mental exertion in the evening to prepare the body for sleep.
In some cases, maintaining good sleep and wake habits can improve sleep issues without the need for medications. Complementary therapies can aid restful sleep. Reflexology and Aromatherapy massage can be beneficial (see our Complementary Therapies factsheet). A few drops of Lavender or Chamomile Pure Essential oil on the pillowcase can be helpful, as can oil burners in the bedroom or Lavender wheat bags warmed in the microwave.
Key points to remember:
- Keep regular sleep times
- Create a restful environment
- Try to exercise regularly
- Try to get fresh air during daylight hours
- Write down or talk about your worries
- Reduce caffeine and alcohol intake
- Seek help from your Doctor if sleep problems continue
If you are having any of the issues mentioned in this factsheet do talk to your Specialist, Parkinson’s Disease Nurse Specialist or one of our MSA Health Care Specialists
Further Information:
https://www.parkinsons.org.uk/information/symptoms/non-motor/sleep
https://britishsnoring.co.uk/about_bssaa.php
https://www.nhs.uk/conditions/sleep-apnoea
https://www.nhs.uk/conditions/restless-legs-syndrome
https://www.sleepfoundation.org/sleep-disorders
https://www.nhs.uk/conditions/urinary-incontinence/treatment
