







People with Multiple System Atrophy (MSA) generally experience urinary problems that may affect the ability to store urine normally or empty the bladder effectively. Symptoms often predate neurological signs of parkinsonism and cerebellar ataxia.
Assessment
The initial assessment of lower urinary tract symptoms should include a dipstick test to rule out a urinary tract infection (UTI) and a bladder scan to assess post micturition residual volume.
Bladder diaries (which should ideally be completed for three days) are a helpful diagnostic tool for the initial assessment as they provide information on fluid intake, number of voids, voided volumes and episodes of incontinence.
Other urological or gynaecological causes for lower urinary tract symptoms such as prostate enlargement should be appropriately ruled out.
Management of lower urinary tract symptoms
- Practical advice should be given about cutting down caffeine, fizzy drinks and alcohol
- Information about timed voiding and bladder retraining whenever appropriate
- The fluid intake should be individualized, particularly taking into consideration possible concurrent cardiac issues. However, a fluid intake of between 1 to 2 litres a day is generally advised
- Catheterization is indicated in individuals with persistently elevated post-void residual volumes in excess of 100-150 ml. Clean intermittent self-catheterisation (CISC) would be the preferable option; this should be taught by a continence specialist nurse . Manual dexterity and the ability to balance when sitting are some of the things that would need to be assessed when considering CISC. With advancing disease, a long-term indwelling catheter may be required, preferably suprapubic rather than urethral
- If patients present with overactive bladder symptoms (frequency, urgency, incontinence) an antimuscarinic medication can be considered, if the person is not retaining urine in their bladder after passing urine. Possibleside-effects might be dry mouth and constipation. If the former is too uncomfortable, artificial saliva may be prescribed. Possible side-effects might be dry mouth and constipation. If the former is too uncomfortable, artificial saliva may be prescribed.
Alternatively, a beta-3 receptor agonist (i.e. mirabegron), could be considered. Mirabegron is generally used at the dose of 50 mg daily; dose adjustments might be required in case of renal or hepatic impairment.
Possible side effects may be hypertension, arrhythmias, headache and gastrointestinal disturbance and the medication is contraindicated in case of severely uncontrolled hypertension.
Referral to specialist urology services would be indicated in cases of haematuria, suspicion of a concomitant urological condition, e.g. prostate enlargement, recurrent urinary tract infections, symptoms refractory to medical management or for consideration of suprapubic catheterisation.
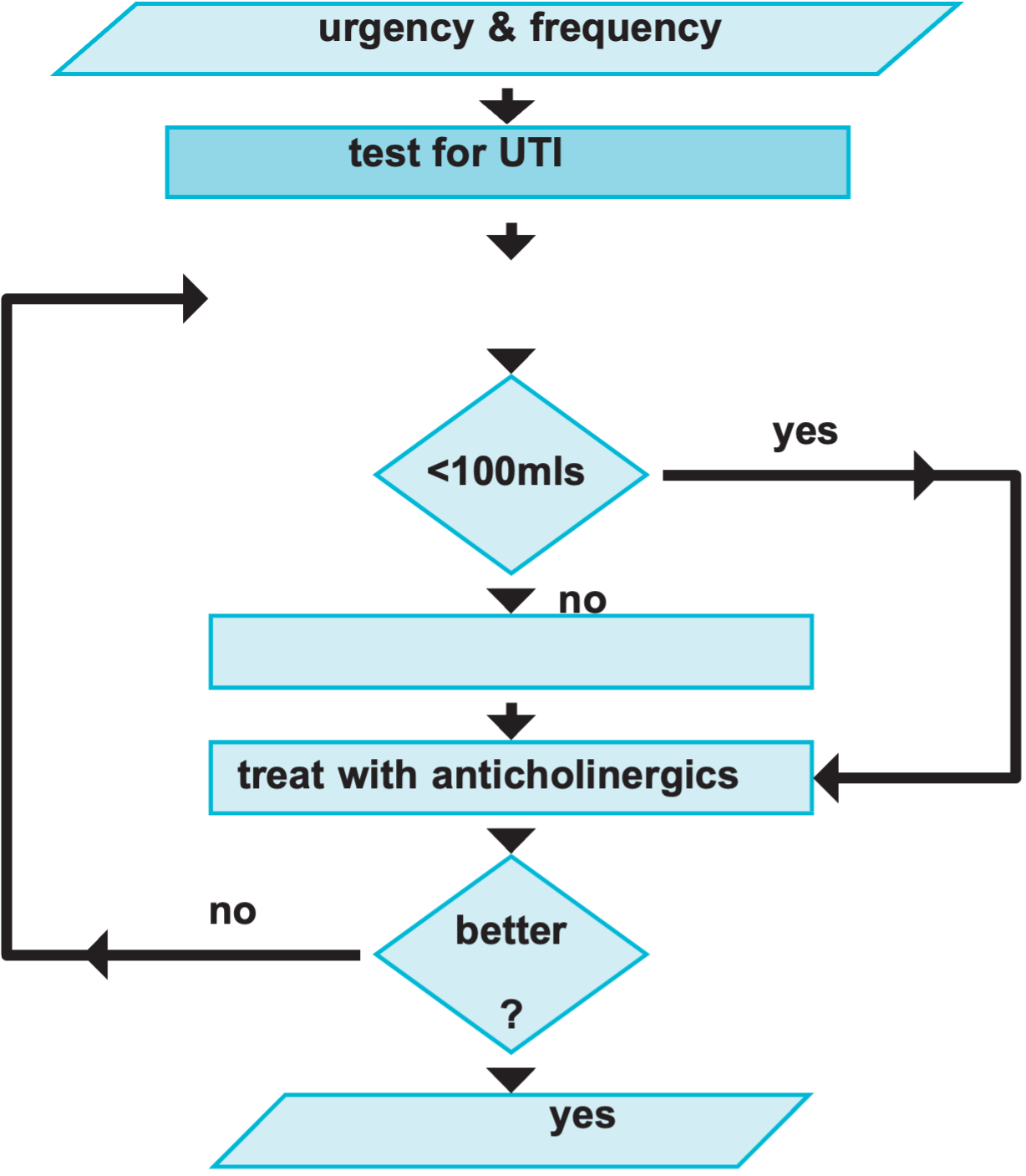
The following is an algorithm for the management of lower urinary tract symptoms:
Management of UTIs
People with MSA who have a UTI may:
- Experience sudden deterioration in core MSA symptoms – e.g. mobility, speech, swallow
- Be prone to uncharacteristic episodes of disorientation +/- hallucinations (not normally part of MSA).
However, people with MSA may not display typical symptoms of a UTI due to the underlying neurological condition e.g:
- May not show signs of a fever
- May not experience discomfort on passing urine
- May not have low back pain.
Abnormalities on urine dipstick testing may be indicative of infection, however a urine sample should be sent for culture and sensitivity when a UTI is suspected. If dipstick is negative in a patient who is symptomatic, we would recommend to still
People with MSA who have a urine infection need:
- Prompt treatment with antibiotics
- Urine sent for culture – treatment changed if required on receipt of culture results
People with MSA who have recurrent urine infections:
- Arrange a bladder scan to check post void residual volume (PVR)
- PVR over 100-150 ml – consider catheterization (CISC / urethral catheterisation/referral for suprapubic catheterisation)
- Further investigating a urological cause (e.g. bladder stones) – ultrasound scan of the kidney and urinary bladder and consider a Urology referral
- Other possible sources of infection should be considered and bowel habits reviewed
- If performing CISC, catheterisation technique should be assessed and optimised if necessary
- May need higher dose of antibiotics for a longer period if they experience recurrent UTIs
- Try cranberry extract tablets or D-Mannose daily
- Try prophylactic methenamine Hippurate (Hiprex) with ascorbic acid
Current literature does not support the routine long-term use of low dose antibiotic prophylaxis due to the lack of efficacy and increase in antimicrobial resistance. If antibiotic prophylaxis is however required under special circumstances, we would suggest choosing three different prophylactic antibiotics according to the results of the urine cultures and to rotate between these antibiotics every six weeks.
You may consider consulting with the local Clinical Microbiology service to discuss prophylactic antibiotics if appropriate.
Our thanks to the Department of Uro-Neurology at The National Hospital for Neurology and Neurosurgery, for their support in creating this resource.
Disclaimer
This factsheet is intended for qualified professionals. The information provided is for guidance purposes only and should be used alongside other relevant research, professional standards and individual clinical or professional judgement. Circumstances for people affected by MSA vary greatly, and professionals should not rely on this material alone when providing support to people.
The resource is produced independently, is not influenced by sponsors and is free from endorsement. References for this information sheet are available by contacting support@msatrust.org.uk.
Your feedback helps us ensure we are delivering information to the highest standard. If you have any comments or suggestions, please contact us at support@msatrust.org.uk.
References
Panicker JN, Fanciulli A, Skoric MK, Kaplan T, Aleksovska K, Adamec I, Averbeck MA, Campese N, Guaraldi P, Leys F, Moreno-Palacios J, Simeoni S, Stankovic I, Wright S, Batla A, Blok B, Hentzen C, Hilz MJ, Kessler TM, Madersbacher H, Nair KR, Nair KPS, Pakzad M, Traon AP, Peryer G, Przydacz M, Sakakibara R, Saraf U, Smith M, Struhal W, Thijs RD, Tudor KI, Tutaj M, Vodušek DB, Wenning G, Habek M. European Academy of Neurology (EAN)/European Federation of Autonomic Societies (EFAS)/International Neuro-Urology Society (INUS) Guidelines for Practising Neurologists on the Assessment and Treatment of Neurogenic Urinary and Sexual Symptoms (NEUROGED Guidelines). Eur J Neurol. 2025 Apr;32(4):e70119. doi: 10.1111/ene.70119.
Heltveit-Olsen SR, Sundvall PD, Gunnarsson R, Snaebjörnsson Arnljots E, Kowalczyk A, Godycki-Cwirko M, Platteel TN, Koning HAM, Groen WG, Åhrén C, Grude N, Verheij TJM, Hertogh CMPM, Lindbaek M, Hoye S. Methenamine hippurate to prevent recurrent urinary tract infections in older women: protocol for a randomised, placebo-controlled trial (ImpresU). BMJ Open. 2022 Nov 1;12(11):e065217. doi: 10.1136/bmjopen-2022-065217. PMID: 36319057.
Tam TY, Aldrich ER, Crisp CC, Yook E, Yeung J, Pauls RN. Methenamine Hippurate With Cranberry Capsules Versus Cranberry Alone for Urinary Tract Infection Prevention in a Short-Term Indwelling Foley Catheter Population After Urogynecologic Surgery: A Double-Blinded Randomized Controlled Trial. Female Pelvic Med Reconstr Surg. 2022 Mar 1;28(3):e55-e61. doi: 10.1097/SPV.0000000000001147. PMID: 35272334.
Salvatore S, Ruffolo AF, Stabile G, Casiraghi A, Zito G, De Seta F. A Randomized Controlled Trial Comparing a New D-Mannose-based Dietary Supplement to Placebo for the Treatment of Uncomplicated Escherichia coli Urinary Tract Infections. Eur Urol Focus. 2023 Jan 6:S2405-4569(22)00297-8. doi: 10.1016/j.euf.2022.12.013. Epub ahead of print. PMID: 36621376.
Phé V, Pakzad M, Haslam C, Gonzales G, Curtis C, Porter B, Chataway J, Panicker JN. Open label feasibility study evaluating D-mannose combined with home-based monitoring of suspected urinary tract infections in patients with multiple sclerosis. Neurourol Urodyn. 2017 Sep;36(7):1770-1775. doi: 10.1002/nau.23173. Epub 2016 Nov 4. PMID: 27813195.
Ledda A, Belcaro G, Dugall M, Riva A, Togni S, Eggenhoffner R, Giacomelli L. Highly standardized cranberry extract supplementation (Anthocran®) as prophylaxis in young healthy subjects with recurrent urinary tract infections. Eur Rev Med Pharmacol Sci. 2017 Jan;21(2):389-393. PMID: 28165546.
Gallien P, Amarenco G, Benoit N, Bonniaud V, Donzé C, Kerdraon J, de Seze M, Denys P, Renault A, Naudet F, Reymann JM. Cranberry versus placebo in the prevention of urinary infections in multiple sclerosis: a multicenter, randomized, placebo-controlled, double-blind trial. Mult Scler. 2014 Aug;20(9):1252