







This document serves as a guide to Occupational Therapists working with people with multiple system atrophy (MSA). It draws on available literature in MSA, Parkinson’s disease and other atypical Parkinsonism disorders. It does not cover aetiology, epidemiology, neuropathology and medical management in any depth. Further reading on these topics and others can be accessed via the list of resources (including the MSA website), given at the end of the document.
The Multiple System Atrophy Trust (MSA Trust) produces a series of specialist MSA factsheets for health professionals to enable them to improve the treatment people with MSA receive.
The Multiple System Atrophy Trust (MSA Trust) is the only charity working in the UK and Ireland specifically to support people with MSA. As well as helping people who have MSA, the Trust supports anyone affected by the disease, including carers, families, friends and health professionals.
The Trust employs MSA Health Care Specialists, manages a telephone and email advice service and runs a network of support groups. We provide up-to-date literature for people affected by MSA and for health professionals. We also fund vital research to find the cause, and one day, cure for MSA.
To ensure services are accessible to everyone, the Trust is committed to providing services for people affected by MSA free of charge. The MSA Trust is a charity funded entirely on voluntary donations.
The MSA Trust is always keen to receive feedback about the information we produce, please email support@msatrust.org.uk with any comments.
Introduction
MSA is a rare progressive neurological disorder that affects adult men and women and leads to premature death. Currently, there is no known cause or cure. MSA causes degeneration or atrophy of nerve cells in several (or multiple) areas of the brain which results in problems with movement, balance and autonomic functions of the body such as swallowing, bowel, bladder and blood pressure control.
Globally, around 4.4 people per 100,000 have MSA which equates to almost 3,300 people living with MSA in the UK [1]. Parkinson’s disease is more common, affecting about 210 per 100,000 in the UK [2].
MSA usually starts between the ages of 50-60 years, but it can affect people younger and older. It affects both sexes [3].
Neuropathology
MSA is an alphasynucelinopathy, presenting pathologically with glial cytoplasmic inclusions and neuronal loss. The mechanisms underlying the condition and the factors that trigger MSA onset are yet to be established. Environmental and dietary influences have been cited [4] however definitive cause and risk factors are yet to be established. Symptoms of MSA are a manifestation of various pathologies originating in the striatonigral, olivopontocerebellar and central autonomic degeneration. This causes a combination of symptoms of Parkinsonism, Cerebellar signs and autonomic dysfunction., as illustrated in Figure 1
![Figure 1 - MSA signs and symptoms (Adapted from Swan [5])](https://www.msatrust.org.uk/wp-content/smush-webp/2026/03/msa-signs-and-symptoms.png.webp)
Clinical Diagnosis of MSA
The term MSA was first used in 1969 – prior to this it had previously been known as Shy -Drager Syndrome. The first diagnostic criteria for MSA were proposed in 1989 [6] and Second Consensus Criteria were defined in 2008 [7] which defined three levels of certainty of the diagnosis—possible, probable and definite MSA. New Movement Disorder Society (MDS) criteria for MSA diagnosis were published in 2022 using an evidence-based and consensus-based methodology [24]. Neuropathologically established MSA criteria remains the same, but new categories of clinically established MSA, clinically probable MSA and possible prodromal MSA are proposed.
Distinguishing MSA from idiopathic Parkinson’s disease is still problematic, with both presenting with abnormal DAT scans. Occupational Therapists need to be aware of clinical features that characteristically distinguish symptoms of MSA from other Parkinsonism syndromes including PD, although these can be hard to discern in the early stages (see Table 1).
The key distinguishing clinical signs at diagnosis are [4]:
- Autonomic failure which includes postural hypotension, bladder and bowel dysfunction, sexual dysfuncion and possible speech and swallow impairment. Poor response to levodopa (may receive transient benefit)
- Akinetic rigid parkinsonism (present in 58% of cases) or cerebellar ataxia (29%)
MSA phenotypes
The criteria used most often to classify MSA recognise two main phenotypes [3]. In general, people present with predominance of Parkinsonian features (MSA-P) or predominance of cerebellar features (MSA-C), however symptoms overlap. Almost all people with MSA develop autonomic symptoms preceded by motor symptoms. In Western hemisphere cohorts approximately 80% of cases are predominantly MSA-P. The contrary is true for Eastern hemisphere populations. This may be due to be to racial genetic differences and cultural characteristics. MSA is a rapidly progressing, multi-organ disorder leading to severe synucleopathy. It has been established that the prognosis is poorer in people who present with early autonomic dysfunction. People who have been classified as MSA-P are more likely to have greater functional decline [8]
MSA-P
The motor symptoms characteristic of MSA-P are similar to those observed in typical Parkinson’s disease and include rigidity, bradykinesia, tremor and poor balance. However, autonomic symptoms can also predate motor symptoms in MSA-P.
MSA-C
Cerebellar symptoms in MSA originate from the trunk spreading to the lower limbs which eventually affect gait. Gait ataxia, limb kinetic ataxia and scanning dysarthria as well as cerebellar occulomotor disturbances are typical motor symptoms of this phenotype.
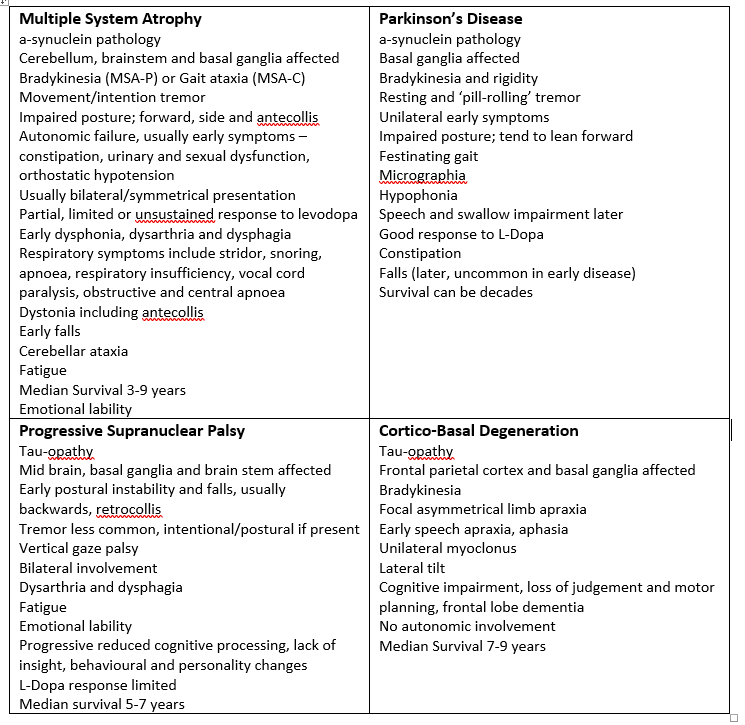
Table 1: Common and distinguishing features for PD, MSA, PSP and CBD (Courtesy of Katie Rigg, MSA Nurse Specialist, Multiple System Atrophy Trust)
Treatment strategies
There is currently no consensus on the stages of disease progression in MSA, nor is it clearly defined. Average survival is close to a decade [8], although this is a guide only. Treatment varies for each stage of the disease and occupational therapists are urged to use their clinical reasoning skills based on the knowledge of the neuropathology of the disease. Forward planning for likely disease trajectory should be incorporated as part of the treatment approach. Person centred goals should be realistic and appropriate, and multi-disciplinary intervention is key to the provision of a quality service.
Management needs to be focussed on quality of life and alleviating symptoms. Regular and frequent review by specialist medical practitioners is required [9]. The table below summarises key medical interventions.
| Symptom | Intervention |
| Parkinsonism | L-Dopa (40-60% of MSA patients will initially respond) |
| Ataxia | Physiotherapy and Occupational therapy |
| Orthostatic hypotension | Non-pharmacological, TEDS, abdominal binder, fluids, small meals, positioning and exercise advice. Pharmacological – fludrocortisone, midodrine, droxidopa. |
| Neurogenic urinary tract dysfunction | Non pharmacological strategies, medications and catheterisation. Urology or continence team involvement. |
| Constipation | Exercise, diet, fluids and medications. Continence team involvement. |
| Erectile dysfunction | Specialist referral to andrology or sexual dysfunction clinic |
| Breathing problems | Physiotherapy, respiratory team, sleep studies, CPAP, tracheostomy |
| Dystonia/pain | Physiotherapy, positioning, support, massage, medications, Botox |
| Camptocormia | Physiotherapy and Occupational therapy support |
| REM Sleep disorder | Sleep studies, clonazepam, melatonin |
| Depression | Non-pharmacological, psychology and psychiatry support, pharmacological interventions |
Table 2: Key symptoms and medical management Adapted from: Flabeau et al [9] andCoon and Ahlskog, 2020 [25].
Occupational Therapy
Occupational therapy adds value to the lives of people with MSA by improving self-perceived performance in daily activities. Occupational therapy aims to make day to day life easier by increasing knowledge around symptom management and by supporting decisions around the choice and timing of equipment, home adaptations and care until the end of life.
There is a growing evidence base from the world of movement disorders and Parkinson’s rehabilitation research [10, 11, 12, 13] to help occupational therapy services strengthen their case towards providing effective services to people and their families throughout their MSA journey.
Primary research regarding the role of occupational therapy with people with MSA is scarce. However, one small pilot randomised control trial [14] found positive benefits of an occupational therapy programme. A subsequent occupational therapy intervention framework was developed from this research [15] providing the first evidence based practical guide for occupational therapists who work with people with MSA.
Other practical clinical guidelines, such as those for people with Parkinson’s [16] and people with Progressive Supranuclear Palsy and Cortico Basal Degeneration [17] are available to help guide occupational therapists when working with people with MSA.
Overarching principles of occupational therapy: anticipating problems before they arise
It is important to remember that MSA is progressive and symptoms can vary on a daily basis.. Although techniques for symptom control in other progressive neurological disorders may prove useful [e.g. for managing fatigue in multiple sclerosis see 19], such techniques should always be used within a client centred context, to avoid treating the symptoms rather than the person.
Additionally, as some people have been misdiagnosed for years prior to an accurate diagnosis of MSA, each person’s understanding of their disease course and resulting stage of emotional acceptance and adjustment of loss of role and function can vary tremendously.
Identifying and anticipating need is critical to optimising quality of life over time. A central role for the Occupational Therapist is helping the person with MSA and their family anticipate day to day problems and find solutions before they occur. Although some people may not be emotionally ready to accept suggestions about their future decline in function, proactive planning of equipment use, the need for a wheelchair or planning a move to single floor living must be placed high on the agenda of every Occupational Therapist to maximise independence and support for both people with MSA and their carers.
Proactive review and open access for when things change unexpectedly should be in place to ensure rapid reassessment is undertaken within the shortest feasible timeframe in addition to overt case coordination and full team case conferences in place. Occupational Therapists should ensure other team members are kept abreast of any plans in place and functional decline, organising joint sessions and accessing other services when required, including proactive involvement and shared working with palliative care teams [20].
Occupational Therapy Assessment and Treatment Interventions
Providing realistic solutions for now and in the future requires an Occupational Therapist to take a flexible client centred approach [15]. Figure 2 provides a dynamic framework to follow, where any change in the person’s goals or need’s triggers a full review.
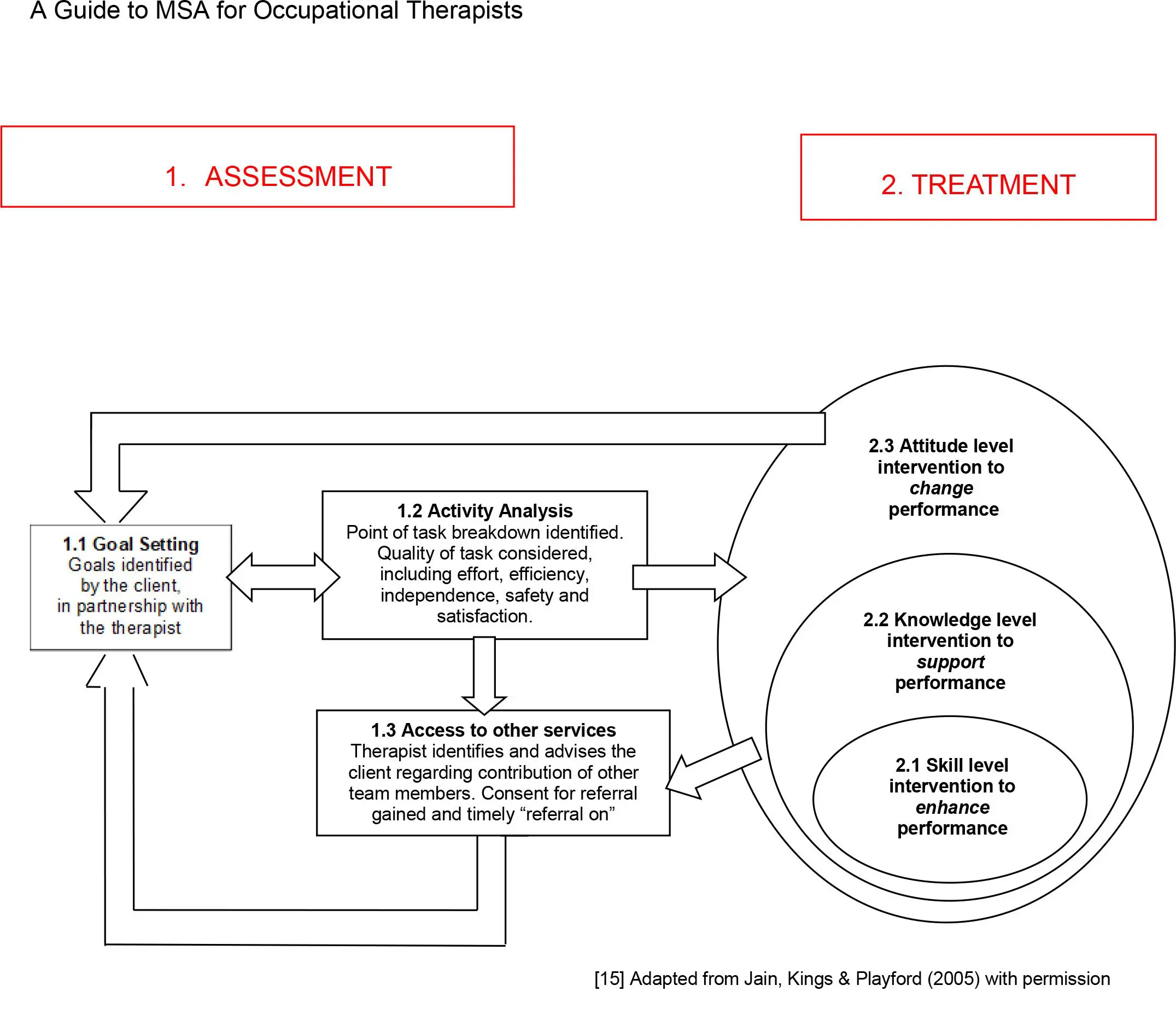
This framework can guide intervention for people at any stage of MSA and enables the person with MSA to work in partnership with the Occupational Therapist, setting goals and taking an active role in all therapy input.
Assessment
Given the rarity of MSA and a sometimes fraught journey to accurate diagnosis and a rapidly declining disease course, Occupational Therapists tend to see people with MSA long after their symptoms have begun.
It is therefore essential that any prior assumptions are set to one side and the process of identifying and meeting unique occupational performance needs is led by the person with MSA and their family.
Goal Setting
Listening to the person’s journey starts the assessment process and underpins all occupational therapy interventions. Where cognitive skills are mainly preserved, the person with MSA should be encouraged to identify their own goals, with the Occupational Therapist just guiding discussions. When features of emotional lability and slowness of thought are demonstrated, the person with MSA should be helped to articulate their goals with support of their family and loved ones or over a longer time period.
In their work in 2005, Jain, Kings & Playford [15] used the Canadian Occupational Performance Measure (COPM) [16, 17] to support the process of identifying and prioritising occupational performance goals. The COPM may also be used as a measure by using visual analogue scales to capture how the person rates the importance of daily tasks and their current satisfaction with their own performance. The use of self-reported disease specific measures such as the Unified Multiple System Atrophy Rating Scale [18] may also prove a useful starting point to identify and prioritise key areas for intervention. Other potential tools include TOMS and AusTOMS, which can be used with other team members to evaluate outcomes, providing more support for service developments.
Activity analysis
Occupational performance should then be assessed to identify where skills during activities of daily living are breaking down. In order to gain the most realistic picture of performance, wherever possible, a range of tasks should be observed in the environment in which they are undertaken and at the appropriate time of day e.g. at home or at someone’s workplace.
Understanding body level changes
In order to effectively analyse task breakdown, it is essential that Occupational Therapists understand what has changed on a body level. This may be different for each person with MSA and this unique combination of body level impairments will underpin a raft of occupational performance problems.
Occupational Therapists should note all changes in the quality of task performance, such as
- effort – more physical or cognitive energy is required during the task
- efficiency – the time taken to perform the task is lengthened
- independence – increasing assistance is needed to ensure task completion
- safety – risks are seen including near misses and actual task breakdown
- satisfaction – task performance is altered and becomes unsatisfactory
It is also essential to reconcile the impairments that MSA brings with other contextual factors such as the influence of:
- time of day on levels of physical and cognitive fatigue
- medication and pain
- mood and emotional adjustment
- social support available
- physical and environmental barriers
Understanding the unique set of body level changes each person is facing and placing these changes in a real life context, will dictate the most useful focus of intervention. Diaries can also be a helpful objective tool to identify particular issues. After a period of activity analysis, the initial goals set should be reviewed realistically, and revised objectives set or gently re-prioritised as required.
Table 2: Body level impairments, occupational performance problems and possible treatment solutions
| Body level impairments | Occupational performance problems | Possible treatment solutions | ||
| Skills | Knowledge | Attitude | ||
| Reduced ability to regulate blood pressure | Unable to get up out of bed without feeling dizzy | Breaking down the physical steps required to move from lying to sitting, using verbal cueing to slow the task down | Information about the use of a mattress elevator, bed rails and profiling bed provided early | Agreement to have a profiling bed plus a hoist for transfers when blood pressure problems are at their worst |
| Ataxia and fatigue of upper limbs | No longer able to use a wet razor to shave due to repeated cuts | Practice using a small table to encourage stability and prop the elbow during shaving | Using an electric razor instead | Discussing the need for a carer to assist with morning routine |
| Stiffness and rigidity on moving | Difficulty getting in and out of a car | Practice getting in and out of the car, staying low to get bottom in first, feet out first | Provision of information about Motability cars including cars that take a wheelchair | Assessment of suitable vehicles and agreement to stay in the wheelchair during car journeys |
| Inability to readily initiate a change in movement | Increasing problems getting up from an armchair during the day | Practice getting in and out of the arm chair with supervision and verbal prompting to get ‘feet first, nose over toes’ | Demonstration of a number of riser recliner armchairs | Acceptance of the need for care during the day and the use of a standing hoist and riser reclining armchair |
| Slowness of thinking and emotional lability | Embarrassment and increasing anxiety when out shopping | Practice planning and sticking to lists when going into shops | Education around the impact of MSA on emotional control | Agreement to have support from a carer when shopping |
| Reduced balance reactions | At risk of tripping and falling when walking | Taping loose carpets and thresholds with zig zag tape to ‘ visually ‘signal’ a change in floor surface | Introduction of a stick for indoor use and trial of mobility scooters while shopping. | Agreement to use a wheelchair for outdoor mobility |
Access to other services
During the assessment phase, Occupational Therapists need to be thinking about accessing the right people, with the right skills and actively involving health and social care teams at the right time. Joint sessions and shared goals with physiotherapy, speech therapy, dietitians and specialist nursing colleagues are essential to meet a person’s needs in the face of rapid functional decline.
Occupational Therapists are central to providing information about the role and contribution of other team members and where possible, should do this before they are needed to ensure enough time is given for the person with MSA and their family to understand and accept support from other services. Occupational Therapists should also be mindful of identifying and meeting the needs of carers through accessing a full carer assessment and facilitating provision of both physical and psychological support including counselling as required.
When accessing other services it is essential that this is done swiftly, with information regarding MSA and its prognosis emphasised. Long waiting lists are frequently encountered when requesting equipment such as a wheelchair or home adaptations, and people with MSA must be recognised as top priority to avoid any delay.
Treatment Phase
Regardless of the stage in the MSA disease journey, Occupational Therapy treatment should aim to increase reported satisfaction in daily tasks [10, 14].
Figure1 illustrates three distinct but interrelated levels of intervention that Occupational Therapists can consider flexibly, towards the overarching outcome of increasing satisfaction with performance.
Skill level intervention to enhance performance
Skill level intervention looks at how the person is undertaking the task, with interventions aimed at reducing the physical or cognitive effort used to optimise or enhance skills.
Skill level treatment includes:
| Technique | Example |
| Hands-on help | Teaching the carer to physically guide weight transference techniques during sit-to-stand to gain ‘nose over toes’ |
| Breaking the task down into smaller steps | Smaller steps of the task are practiced to slow the task down, with physical help, verbal prompting or equipment added in to reduce task effort |
| Optimising the environment | This includes the addition of lighting in dark or troublesome areas of the house Securing loose floor surfaces and providing grab rails Using hazard tape to draw cognitive attention to the need to change direction or walking speed at door thresholds |
| External and self cueings | Cueing technique, such as extrinsic visual cue cards such as ‘feet first’ and intrinsic such as ‘large steps’ [16], may be useful for people with MSA-P to gain more control over the flow of movement. |
Knowledge level intervention to support performance
Supporting performance by increasing knowledge is a powerful intervention for occupational therapists to use. Whilst not aiming to change how the task is done, education and information can help the person understand why the task is breaking down so that s/he can make informed choices regarding options to support their performance
Knowledge level treatment includes
| Technique | Example |
| Education about symptom management | Providing details about how MSA progresses Providing guidance about the use and timing of medication Keeping a fatigue diary and understanding how to proactively manage fatigue |
| Information about equipment options | Providing information regarding the choice and use of small pieces of equipment Discussing how to get the process of major adaptations at home underway before the disease progresses Knowing how to hire a shop-mobility scooter whilst shopping |
| Providing help to stay in work | Discussing legal rights and available support to stay in work |
| Providing information about other services | Introducing other services and the role they play including help at home from carers, support for families, palliative care services, respite and hospice care |
Attitude level intervention to change performance
Attitude level intervention is possible when the person with MSA understands what point they have reached regarding emotional and practical acceptance of their disease. This includes knowing what has changed at a body level and understanding how this impacts on the quality of task performance, combined with the right information to make informed choices.
Helping support attitudinal level change requires the occupational therapist to work alongside the person with MSA and their family towards a different set of expectations. This may include discussing how the nature of a task could be changed completely achieving the same goal with less effort or major lifestyle changes such as accepting care or moving home. Attitude level treatment includes
| Technique | Example |
| Changing the way the task is performed | Buying pre-prepared meals to avoid cooking from scratch Using a scooter to mobilise safely outdoors |
| Removing the need to do a task | Ordering shopping on-line and having it delivered Paying for a gardener or cleaner Deciding to accept medical retirement |
| Accepting more care and support | Accepting the need for care and equipment at home Understanding when residential or hospice care might be the safest place to live |
Occupational therapy in action: Case examples
These case examples aim to illustrate the type of goals people with MSA might articulate and how Occupational Therapist might plan their treatment, including the role and function of other team members.
Bob: a 66 year old man with a diagnosis of MSA-P
| Goal: to reduce effort and increase safety with bath transfers | ||||
| Activity analysis | Skills | Knowledge | Attitude | Referrals made |
| Problems due to – increasing stiffness and rigidity – reduced balance reactions – increasing episode of ‘freezing’ leading to – anticipatory anxiety when bathing | Practicing – a step by step way of getting into and out of the bottom of the bath – using visual prompt cards – and verbal cueing from wife to guide movement | Providing information regarding – the need for grab rails by the bath – use of a swivel bather or bath lift – installation of a level access shower – the need to have the bathroom door open outwards in the event of a fall | Discussing options regarding – providing paid for care to assist with morning routine – anticipatory discussion regarding moving to single storey living | Physiotherapist for stiffness and rigidity Social Services OT for equipment provision Social Work Team for future care provision |
Phil: 59 year old man diagnosed with MSA-P
| Goal: to optimise comfort and relieve carer burden | ||||
| Activity analysis | Skills | Knowledge | Attitude | Referrals made |
| Problems due to – rapid physical decline including trunk and limb rigidity – persistent hypotension – inability to take weight through lower limbs during transfers – declining respiratory function | Practicing with the wife and care team – the use of a hoist for all transfers – changing position in bed to optimise respiratory function whilst accommodating hypotension | Providing information regarding – identifying the symptoms of sudden low blood pressure and respiratory distress – the need for a pressure mattress and profiling hospital bed | Discussing options regarding – the purpose of an advanced directive – hospice at home and palliative care support | Palliative Care review including assessment of respiratory and hypotension status and mobilising hospice at home services. Urgent District Nursing input regarding declining physical status and the need to access a hospital bed and pressure mattress |
Barbara: a 49 year old lady with MSA-C
| Goal: to reduce fatigue and increase satisfaction with daily energy levels | ||||
| Activity analysis | Skills | Knowledge | Attitude | Referrals made |
| Problems due to – trunkal instability – increasingly unsteady gait – reduced coordination of finer skilled movements | Practising – reducing effort during personal care and domestic routines by sitting when possible to undertake tasks – reducing unwanted excursion of hands by elbow propping during finer skilled tasks | Providing information regarding – fatigue management techniques including the need for proactive rest – using a motorised scooter to get to work rather than struggling to walk outdoors | Discussing options regarding – applying for any benefit entitlement to help pay for domestic support at home or taxis – raising the option of working from home with employer | Physiotherapist for ataxia and core stability Disability Employment Advisor for support via the ‘Access to Work’ scheme Citizens Advice Bureau or MSA Trust Social Welfare Specialist regarding benefit entitlement |
[15] Adapted from Jain, Kings & Playford (2005) with permission
End of Life Care: The Occupational Therapist’s role
Every Occupational Therapist has an active role to play in preparing the person with MSA and their family for functional decline towards death. Significant and life changing decisions need to be raised and discussed as early as acceptable, so people have time to understand and accept change and decline over time. Major adaptions at home need to be considered and undertaken early and discussions around where the person wants to die raised and plans put in place.
Identifying and meeting the needs of carers is critical, with Occupational Therapists playing a central role in assessing carer burden with the aim of facilitating additional support to avoid carers reaching breaking point at home. Occupational Therapists should discuss accessing family counselling for spouse or partner and children, and keep a frequent dialogue open about the need for formal care, including options for respite, residential care and hospice support. Alongside members of the wider team including equipment providers, MSA Health Care Specialists, district nursing and palliative care colleagues, Occupational Therapists should guide decision making with realistic and feasible options to maintain goals where possible, relieve suffering and optimise effective end of life care.
Written by Northern Neurological Alliance with Jill Kings (nee Dawson)
Disclaimer
This factsheet is intended for qualified professionals. The information provided is for guidance purposes only and should be used alongside other relevant research, professional standards and individual clinical or professional judgement. Circumstances for people affected by MSA vary greatly, and professionals should not rely on this material alone when providing support to people.
The resource is produced independently, is not influenced by sponsors and is free from endorsement. References for this information sheet are available by contacting support@msatrust.org.uk.
Your feedback helps us ensure we are delivering information to the highest standard. If you have any comments or suggestions, please contact us at support@msatrust.org.uk.
References:
1. A Schrag, Y Ben-Shlomo, and NP Quinn Prevalence of progressive supranuclear palsy and
multiple system atrophy; a cross sectional study. Lancet. 2006; 354: 1771-1775
2. Parkinsons website http://www.parkinsons.org.uk/content/what-parkinsons
3. GK Wenning and F Krismer Multiple System Atrophy; Chapter in Oxford Textbook of
Movement Disorders. 2013. Ed D Burn; Series Ed C Kennard
4. PA Hanna, JJ Jankovic, and JB Kirkpatrick Multiple System Atrophy: The putative causative
role of environmental toxins. Arch Neuro 1999; 56:90 – 4
5. L Swan and J Dupont Multiple System Atrophy. Physical Therapy. 1999. 79:488-494.
6. S Gilman, PA Low, N Quinn et al. Consensus statement on the diagnosis of multiple
system atrophy. J Auton Nerv Syst 1998.74:189–92.
7. S Gilman, GK Wenning, et al. Second consensus statement on the diagnosis of multiple
system atrophy. Neurology. 2008; 71: 670-676.
8. GK Wenning, F Gesser, et al The natural history of Multiple System Atrophy: a prospective
European cohort study. Lancet Neurol. 2013. 12: 264-74.
9. O Flabeau, G Meissner, and F Tison. Multiple System Atrophy: current and future
approaches to management. Therapeutic Advances in Neurological Disorders. 2010;
3(4):249-263.
10. I.H.W.M.,Sturkenboom, M.J.L., Graff, J C.M., Hendriks, Y., Veenhuizen, M., Munneke, B.R., Bloem, M.W,Nijhuis-van der Sanden, Efficacy of occupational therapy for patients with Parkinson’s disease: A randomised controlled trial. The Lancet Neurology. 2014.13(6): 557-566.
11. E.R., Foster, M.Bedekar, & L Tickle-Degnen, (2014) Systematic review of the effectiveness of occupational therapy-related interventions for people with Parkinson’s disease. American Journal of Occupational Therapy.2014. 68: 39-49.
12. A Aragon, J Kings & ED Playford. The role of the occupational therapy in the rehabilitation of people with movement disorders, in Rehabilitation for Movement Disorders, ed. Lansek R & Morris, ME. Cambridge University Press. 2013. Cambridge.
13. J Jansa, A Aragon & A Lundgren-Nilsson. How People Living with Parkinson’s Disease in Four European Countries View Occupational Therapy. The European Neurological Journal 3. 2011. pp. 1-7
14. S Jain, J Dawson, NP Quinn & E D Playford.. Occupational therapy in multiple system atrophy: a pilot randomised controlled trial. Movement Disorders. 19 (11). 2004. pp.1360–1364.
15. S Jain, J Kings, E D Playford. Occupational Therapy for people with Progressive Neurological Disorders: Unpacking the Black Box. Br.J. Occ. Th. 68 (3) 2005. pp. 125-130.
16. A Aragon & J Kings. Occupational Therapy for People with Parkinson’s: Best practice guidelines. 2010. College of Occupational Therapists, London.
17. PSP Association. A guide for PSP and CBD for Occupational Therapists.2013. Northampton http://www.pspassociation.org.uk/wp-content/uploads/2012/07/PSPA-OT-Guide-2013-web.pdf?5d9d2d Accessed 01.07.15.
18. R Silva, J Saute, A Silva, M Coutinho, M Srariva-Pereira & L Jardim. Occupational therapy in spinocerebellar ataxia type 3: an open-label trial. Braz J Med Biol Res, 43 (6).2010. pp. 537-542.
19. S Harrison. Fatigue management for people with multiple sclerosis. 2nd edition. College of Occupational Therapist. 2007. London.
20. L Turner-Stokes, N Sykes, E Silber, A Khatri, L Sutton & E Young. From diagnosis to death: exploring the interface between neurology, rehabilitation and palliative care in managing people with long-term neurological conditions. Clinical Medicine. 7(2). 2007.pp. 129 – 136.
21. M Law, S Baptiste, A Carswell, MA McColl, H Polatajko, & N Pollock. Canadian Occupational Performance Measure (4th edition). 2005. Canadian Association of Occupational Therapists. Ottawa, Ontario.
22. M Law, S Baptiste, M McColl, A Opzoomer, H Polatajko, N Pollock. The Canadian occupational performance measure: an outcome measure for occupational therapy. Canadian Journal of Occupational Therapy, Revue Canadienne d Ergotherapie 57(2).1990.pp. 82-7.
23. GK Wenning, F Tison, K Seppi, C Sampaio, A Diem, F Yekhlef, I Ghorayeb, F Ory, M Galitzky, T Scaravilli, M Bozi, C Colosimo, S Gilman, CW Shults, NP Quinn, O Rascol,W Poewe and the Multiple System Atrophy Study Group () Development and validation of the Unified Multiple System Atrophy Rating Scale (UMSARS) Movement Disorders. 19 (12). 2004. pp. 1391 -1402.
24. Wenning GK, Stankovic I, Vignatelli L, Fanciulli A, Calandra-Buonaura G, Seppi K, Palma JA, Meissner WG, Krismer F, Berg D, Cortelli P, Freeman R, Halliday G, Höglinger G, Lang A, Ling H, Litvan I, Low P, Miki Y, Panicker J, Pellecchia MT, Quinn N, Sakakibara R, Stamelou M, Tolosa E, Tsuji S, Warner T, Poewe W, Kaufmann H. The Movement Disorder 10.1002/mds.29005. Epub ahead of print. PMID: 35445419
25. My Treatment Approach to Multiple System Atrophy (mayoclinicproceedings.org) accessed October 2022. Full reference My Treatment Approach to Multiple System Atrophy – Mayo Clinic Proceedings